Deep within our bones lies one of the body’s most remarkable and essential organs—bone marrow. Often overlooked, this soft, spongy tissue functions as a sophisticated biological factory that continuously produces billions of blood cells every day. These cells are responsible for carrying oxygen throughout the body, fighting infections, and preventing excessive bleeding. Without healthy bone marrow, life-sustaining processes quickly begin to break down.
When bone marrow fails to produce blood cells normally or begins generating abnormal cells, a wide range of conditions known as bone marrow disorders can develop. Some disorders result in dangerously low blood cell counts, while others cause uncontrolled production of abnormal cells that can interfere with normal body functions. In severe cases, these conditions may progress to life-threatening blood cancers or lead to significant complications affecting multiple organs.
Bone marrow disorders encompass a diverse group of diseases, ranging from relatively rare bone marrow failure syndromes to more common conditions such as leukemia and multiple myeloma. While some are inherited through genetic mutations, many develop later in life due to environmental exposures, immune system dysfunction, infections, or age-related changes in the blood-forming system.
Advances in modern medicine have transformed the diagnosis and treatment of many bone marrow disorders. Sophisticated laboratory testing, molecular diagnostics, targeted therapies, immunotherapy, and stem cell transplantation have significantly improved outcomes for many patients. However, early recognition remains critical because timely diagnosis often allows for more effective treatment and better long-term prognosis.
Understanding how bone marrow functions, recognizing the warning signs of disease, and becoming familiar with available treatment options can empower patients and families to seek appropriate medical care when needed. This comprehensive guide explores the major types of bone marrow disorders, their causes, symptoms, diagnosis, treatment approaches, and the latest advances offering hope to those affected by these complex conditions.
Why Bone Marrow Disorders Matter More Than Many People Realize
For many individuals, the earliest signs of a bone marrow disorder may appear subtle—persistent fatigue, recurrent infections, easy bruising, or unexplained weakness. Because these symptoms often resemble common illnesses or age-related changes, diagnosis can sometimes be delayed. Yet beneath these seemingly minor symptoms may lie a disorder affecting the body’s entire blood-forming system.
Bone marrow disorders are significant because they impact the production of every major blood cell type required for survival. Left untreated, some conditions can lead to severe anemia, life-threatening infections, dangerous bleeding complications, organ damage, or progression to aggressive blood cancers. Early recognition and prompt medical evaluation can dramatically improve outcomes, making awareness an essential component of disease prevention and management.
The Hidden Factory Inside Your Bones
Although bones are commonly associated with providing structure and protection, many contain a highly active tissue known as bone marrow. Found primarily within the pelvis, ribs, breastbone, spine, and long bones, bone marrow serves as the body’s primary blood cell production center.
There are two major types of bone marrow. Red marrow is responsible for producing blood cells and contains hematopoietic stem cells—the specialized cells capable of developing into all types of mature blood cells. Yellow marrow primarily consists of fat cells and functions as an energy reserve, although it can convert back to red marrow under certain circumstances when increased blood production is required.
At the heart of this system are hematopoietic stem cells. These extraordinary cells continuously divide and mature into three major blood cell categories:
• Red blood cells, which transport oxygen from the lungs to tissues throughout the body.
• White blood cells, which form a critical component of the immune system and help defend against infections.
• Platelets, which assist in blood clotting and help prevent excessive bleeding following injury.
The process of blood cell formation, known as hematopoiesis, occurs continuously throughout life. Every second, millions of new blood cells are generated to replace aging cells that naturally die and are removed from circulation. This finely regulated process ensures that the body maintains an adequate supply of healthy blood cells to meet its ongoing needs.
When bone marrow functions normally, blood cell production remains balanced and efficient. However, disruptions affecting stem cells, the marrow environment, or the genetic instructions governing blood cell development can lead to significant abnormalities. These abnormalities form the basis of many bone marrow disorders.
What Are Bone Marrow Disorders?
Bone marrow disorders are conditions that impair the marrow’s ability to produce healthy blood cells or cause the production of abnormal blood cells. These disorders can affect one or more blood cell lines and vary considerably in severity, ranging from mild abnormalities detected during routine testing to aggressive diseases requiring urgent medical intervention.Some bone marrow disorders originate directly within the marrow itself. In these conditions, stem cells or developing blood cells acquire genetic abnormalities that interfere with normal maturation and growth. Examples include myelodysplastic syndromes, myeloproliferative neoplasms, leukemia, and multiple myeloma.
Other disorders develop when diseases originating elsewhere in the body spread to the bone marrow. Certain cancers, autoimmune diseases, infections, and metabolic disorders can infiltrate or damage marrow tissue, impairing its ability to function properly.
The consequences of abnormal blood cell production depend on which cell types are affected. Reduced red blood cell production can cause anemia and fatigue. Low white blood cell counts increase susceptibility to infections. Platelet deficiencies may result in bruising and dangerous bleeding complications. In some cases, excessive production of abnormal blood cells can crowd out healthy cells and disrupt multiple organ systems.
How Bone Marrow Disorders Are Classified
Bone marrow disorders are commonly classified according to their underlying mechanisms and effects on blood cell production.
Some disorders cause decreased blood cell production. Conditions such as aplastic anemia and certain bone marrow failure syndromes reduce the marrow’s ability to generate adequate numbers of healthy blood cells, leading to anemia, infections, and bleeding complications.
Others cause excessive blood cell production. Myeloproliferative neoplasms, for example, result in overproduction of one or more blood cell types. Although blood counts may appear elevated, the cells produced are often abnormal and may not function properly.
A separate category includes bone marrow cancers and blood cancers. Leukemia, multiple myeloma, and certain lymphomas arise from abnormal blood-forming cells that proliferate uncontrollably within the marrow.
Bone marrow infiltration disorders occur when cancer cells, infections, fibrosis, or other abnormal substances invade the marrow space and interfere with normal blood formation.
Additionally, bone marrow disorders may be classified as inherited or acquired. Inherited disorders result from genetic abnormalities present from birth, whereas acquired disorders develop later due to environmental factors, immune system dysfunction, infections, or spontaneous genetic mutations.
Major Types of Bone Marrow Disorders
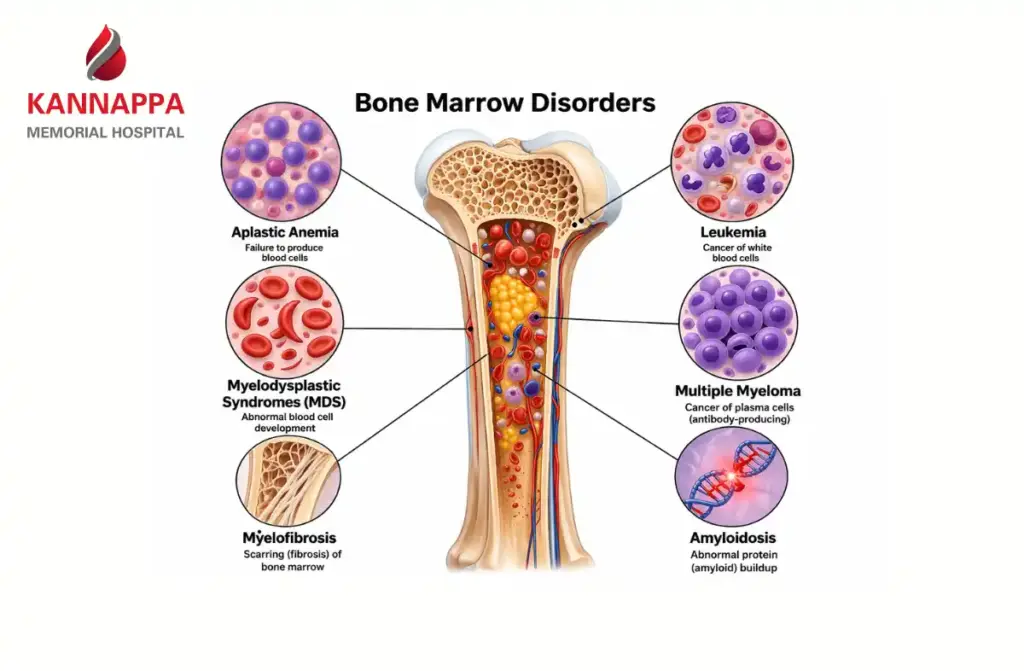
- Aplastic anemia is a rare but serious condition in which the bone marrow fails to produce sufficient red blood cells, white blood cells, and platelets. Patients often experience fatigue, recurrent infections, and increased bleeding tendencies.
- Myelodysplastic syndromes (MDS) involve ineffective blood cell production caused by abnormal stem cell development. Although the marrow may appear active, many developing cells die before reaching maturity, resulting in low blood counts and an increased risk of progression to leukemia.
- Myeloproliferative neoplasms (MPNs) are characterized by excessive production of blood cells. Examples include polycythemia vera, essential thrombocythemia, and primary myelofibrosis.
- Leukemia develops when abnormal white blood cells proliferate uncontrollably within the bone marrow and bloodstream. Depending on the specific subtype, leukemia may progress rapidly or slowly.
- Multiple myeloma is a cancer of plasma cells, specialized immune cells responsible for antibody production. The disease can weaken bones, impair kidney function, and suppress normal blood cell production.
- Myelofibrosis involves progressive scarring of bone marrow tissue, reducing its ability to produce healthy blood cells and often causing enlargement of the spleen.
- Bone marrow failure syndromes represent a group of inherited and acquired disorders characterized by inadequate blood cell production. Examples include Fanconi anemia and dyskeratosis congenita.
- Secondary bone marrow disorders can result from autoimmune diseases, severe infections, metastatic cancers, nutritional deficiencies, and exposure to toxic substances or medications.
Common Causes and Risk Factors
- Bone marrow disorders can arise from a complex interaction of genetic, environmental, immune-related, and age-associated factors. In many patients, the exact cause remains unknown. However, several well-established risk factors have been identified.
- Inherited genetic mutations can increase susceptibility to bone marrow failure syndromes and certain blood cancers. Conditions such as Fanconi anemia, Shwachman-Diamond syndrome, and dyskeratosis congenita are examples of inherited disorders that directly affect bone marrow function.
- Autoimmune diseases may cause the immune system to mistakenly attack bone marrow stem cells, leading to reduced blood cell production. This mechanism is particularly important in some cases of aplastic anemia.
- Exposure to ionizing radiation is another recognized risk factor. High-dose radiation can damage bone marrow cells and increase the likelihood of developing blood disorders years after exposure.
- Certain chemicals, especially benzene, have been strongly linked to bone marrow damage and leukemia. Occupational exposure in industries involving petroleum products, paints, solvents, and chemical manufacturing may increase risk when appropriate safety measures are not followed.
- Some medications and cancer treatments can suppress bone marrow activity. Chemotherapy and radiation therapy, while essential for treating many cancers, can temporarily or permanently affect blood cell production.
- Viral infections such as hepatitis viruses, Epstein-Barr virus, parvovirus B19, and HIV have also been associated with certain bone marrow disorders. These infections may directly damage marrow cells or trigger abnormal immune responses.
- Advancing age remains one of the most significant risk factors for many acquired bone marrow disorders, particularly myelodysplastic syndromes, leukemia, and multiple myeloma. As people age, accumulated genetic changes within stem cells can increase the likelihood of disease development.
Understanding the Role of Genetic Mutations
Recent advances in molecular medicine have revealed that many bone marrow disorders are driven by specific genetic mutations within blood-forming stem cells. These mutations are usually acquired during life rather than inherited from parents.
Examples include mutations involving:
• JAK2, CALR, and MPL genes in myeloproliferative neoplasms
• TP53, ASXL1, TET2, and DNMT3A mutations in myelodysplastic syndromes and leukemia
• Various chromosomal abnormalities associated with leukemia and multiple myeloma
Identifying these genetic changes has become increasingly important because they help physicians establish diagnoses, predict disease behavior, assess prognosis, and select targeted therapies tailored to individual patients.
Early Warning Signs You Should Never Ignore
- Because bone marrow disorders interfere with blood cell production, symptoms often develop gradually and may initially be mistaken for common illnesses or aging-related changes. Recognizing early warning signs can lead to earlier diagnosis and improved treatment outcomes.
- Persistent fatigue is among the most common symptoms. Individuals may feel unusually tired despite adequate rest and may struggle with routine activities that were previously manageable.
- Frequent or unusually severe infections can indicate a deficiency of functional white blood cells. Recurrent respiratory infections, prolonged fevers, or infections that are difficult to treat warrant medical evaluation.
- Easy bruising, frequent nosebleeds, bleeding gums, or prolonged bleeding from minor cuts may suggest low platelet counts. These symptoms often indicate impaired clotting function.
- Shortness of breath, dizziness, headaches, and reduced exercise tolerance commonly occur when anemia limits oxygen delivery throughout the body.
- Many patients develop pale skin due to decreased red blood cell production. This symptom may be particularly noticeable in the face, palms, or inside the lower eyelids.
- Bone and joint pain can occur in conditions where abnormal cells accumulate within the marrow. This symptom is especially common in leukemia and multiple myeloma.
- Some disorders may cause enlargement of lymph nodes, the liver, or the spleen. Patients may notice swelling in the neck, underarms, or abdomen.
- Unexplained weight loss, persistent fevers, and night sweats can signal more advanced disease and should never be ignored.
How Bone Marrow Disorders Affect the Blood
The effects of bone marrow disorders largely depend on which blood cell populations are affected. Since bone marrow produces all major blood cells, abnormalities can have widespread consequences throughout the body.
Effects on Red Blood Cells
- Red blood cells transport oxygen from the lungs to tissues and organs. When bone marrow cannot produce enough healthy red blood cells, anemia develops.
- Anemia reduces oxygen delivery throughout the body, causing fatigue, weakness, shortness of breath, dizziness, headaches, and decreased physical endurance. Severe anemia may place additional strain on the heart and cardiovascular system as the body attempts to compensate for reduced oxygen availability.
Effects on White Blood Cells
- White blood cells form a crucial component of the immune system. Reduced production of these cells weakens the body’s ability to fight infections.
- Patients with low white blood cell counts may experience recurrent bacterial, viral, or fungal infections. Even minor infections can become serious when immune defenses are compromised.
- In some disorders, white blood cell numbers may be elevated, but the cells themselves function abnormally. Despite high counts, patients remain vulnerable to infection because the cells cannot effectively protect the body.
Effects on Platelets
- Platelets play a vital role in blood clot formation. Insufficient platelet production increases the risk of bleeding complications.
- Common manifestations include easy bruising, petechiae (tiny red or purple skin spots), nosebleeds, bleeding gums, heavy menstrual bleeding, and prolonged bleeding after injury or surgery.
- In severe cases, dangerously low platelet counts can result in life-threatening internal bleeding.
Potential Complications of Abnormal Blood Counts
When blood cell abnormalities persist untreated, significant complications can develop. Chronic anemia may lead to cardiovascular stress and reduced organ function. Recurrent infections can become severe or life-threatening. Platelet deficiencies increase bleeding risks, while abnormal blood cell proliferation can damage tissues and organs throughout the body.
Complications of Untreated Bone Marrow Disorders
- Without appropriate treatment, many bone marrow disorders progressively worsen over time.
- Severe anemia can place substantial strain on the heart, potentially contributing to heart failure in vulnerable individuals. Chronic oxygen deprivation may impair the function of multiple organs and significantly reduce quality of life.
- Persistent immune dysfunction increases susceptibility to serious infections that may require hospitalization and intensive treatment.
- Bleeding complications can range from recurrent minor bruising to major hemorrhages involving the gastrointestinal tract, lungs, or brain.
- Certain disorders, particularly myelodysplastic syndromes and some myeloproliferative neoplasms, may transform into acute leukemia, a more aggressive form of blood cancer requiring intensive treatment.
- Progressive fatigue, weakness, pain, and declining physical function can significantly affect daily activities, emotional well-being, and overall quality of life.
Diagnostic Tests and Evaluation
- Accurate diagnosis is essential because treatment strategies vary considerably among different bone marrow disorders. Physicians typically use a combination of clinical assessment, laboratory testing, and specialized diagnostic procedures.
- The evaluation usually begins with a detailed medical history and physical examination. Physicians assess symptoms, family history, occupational exposures, medication use, and any previous medical conditions that may contribute to bone marrow dysfunction.
- A Complete Blood Count (CBC) is often the first diagnostic test performed. This test measures red blood cells, white blood cells, hemoglobin levels, and platelet counts, providing valuable clues regarding underlying abnormalities.
- A peripheral blood smear allows specialists to examine blood cells under a microscope. Changes in cell size, shape, or maturity can provide important diagnostic information.
- Reticulocyte counts help determine whether the bone marrow is producing new red blood cells appropriately.
- Additional laboratory studies may evaluate vitamin deficiencies, autoimmune disorders, infections, and other conditions that can affect blood production.
- For many patients, a bone marrow aspiration and biopsy remain the most important diagnostic procedures. These tests provide direct information about marrow cellularity, blood-forming activity, and the presence of abnormal cells.
- Advanced diagnostic techniques have become increasingly important in modern hematology. Cytogenetic testing identifies chromosomal abnormalities associated with specific diseases, while molecular and genetic testing can detect mutations that guide diagnosis, prognosis, and treatment selection.
- Flow cytometry helps classify abnormal blood cells and is particularly valuable in diagnosing leukemia, lymphoma, and related disorders.
- Imaging studies such as CT scans, MRI scans, and PET scans may be recommended when physicians need to evaluate lymph nodes, organs, or bone involvement.
Why Early Diagnosis Can Change Outcomes
- Early diagnosis is one of the most important factors influencing treatment success in many bone marrow disorders. Detecting disease before severe complications develop allows healthcare providers to intervene earlier, monitor disease progression more effectively, and implement therapies that may prevent irreversible damage.
- For patients with blood cancers, early diagnosis may improve treatment response and long-term survival. In bone marrow failure disorders, timely intervention can reduce the risk of severe infections, bleeding episodes, and organ complications.
- Routine blood testing often provides the first indication that a bone marrow disorder may be present. Even mild abnormalities in blood counts should be evaluated carefully when they persist or cannot be explained by common medical conditions.
Understanding Bone Marrow Biopsy
- A bone marrow biopsy is one of the most valuable diagnostic tools for evaluating bone marrow disorders. While many patients feel anxious when the procedure is recommended, understanding what it involves can help reduce uncertainty and improve preparation.
- Doctors typically recommend a bone marrow biopsy when blood tests reveal unexplained abnormalities, such as persistent anemia, low white blood cell counts, low platelet counts, or unusually high blood cell levels. The procedure is also essential for diagnosing and monitoring conditions such as leukemia, myelodysplastic syndromes, multiple myeloma, aplastic anemia, and myeloproliferative neoplasms.
- Most bone marrow biopsies are performed using the back of the hip bone (posterior iliac crest). During the procedure, local anesthesia is used to numb the area. A small sample of liquid marrow (aspiration) and a small core of bone marrow tissue (biopsy) are collected for laboratory analysis. Although patients may feel pressure or brief discomfort, the procedure is generally well tolerated and typically takes less than 30 minutes.
- Recovery is usually straightforward. Mild soreness at the biopsy site may persist for a few days, but most individuals can resume normal activities shortly afterward. The information obtained from the biopsy helps physicians determine the exact diagnosis, assess disease severity, identify genetic abnormalities, and develop an individualized treatment plan.
Treatment Options for Bone Marrow Disorders
Treatment depends on the specific disorder, disease severity, age, overall health, and individual patient factors. Modern treatment strategies often combine supportive care, medications, and advanced therapies to improve outcomes and quality of life.
Supportive Care
- Supportive treatments play a critical role in managing symptoms and preventing complications.
- Blood transfusions may be required to treat significant anemia and improve oxygen delivery throughout the body. Patients often experience increased energy levels and reduced symptoms following transfusion.
- Platelet transfusions can help prevent or control bleeding in individuals with dangerously low platelet counts.
- Prompt identification and treatment of infections are essential, particularly for patients with weakened immune systems. Antibiotics, antiviral medications, and antifungal therapies may be used when necessary.
Medication-Based Treatments
- Several medications can stimulate blood cell production or target the underlying disease process.
- Growth factor therapies encourage the bone marrow to produce additional red blood cells or white blood cells. These medications can reduce transfusion requirements and lower infection risk in selected patients.
- Immunosuppressive medications are commonly used in disorders such as aplastic anemia, where the immune system contributes to marrow damage.
- Targeted therapies have transformed the treatment landscape for many bone marrow disorders. These medications specifically attack abnormal cellular pathways while minimizing damage to healthy cells.
- Chemotherapy remains an important treatment option for various leukemias and aggressive bone marrow cancers. Treatment protocols vary depending on the disease subtype and individual patient characteristics.
- Precision medicine approaches increasingly allow physicians to tailor treatments based on specific genetic mutations and molecular abnormalities identified through advanced testing.
Advanced Treatment Options
For certain patients, stem cell transplantation offers the possibility of long-term disease control or cure.
Clinical trials also provide access to promising new therapies and continue to advance the understanding and treatment of bone marrow disorders. Patients may benefit from discussing trial opportunities with their healthcare team when appropriate.
Bone Marrow Transplant: A Potential Lifesaving Treatment
- A bone marrow transplant, more accurately called a hematopoietic stem cell transplant, replaces diseased or damaged bone marrow with healthy blood-forming stem cells.
- This procedure may be recommended for conditions such as severe aplastic anemia, acute leukemia, certain myelodysplastic syndromes, multiple myeloma, and some inherited bone marrow failure syndromes.
- There are two primary transplant types. In an autologous transplant, a patient’s own stem cells are collected, stored, and later reinfused after intensive treatment. In an allogeneic transplant, stem cells are obtained from a compatible donor.
- Successful donor selection depends heavily on Human Leukocyte Antigen (HLA) matching. Close matches reduce the risk of complications and improve transplant outcomes.
- Although transplantation can be lifesaving, it carries significant risks, including infection, graft-versus-host disease, organ complications, and treatment-related side effects. Careful patient selection and comprehensive follow-up are essential.
- Recovery often occurs gradually over several months. Patients require ongoing monitoring to assess immune recovery, detect complications, and ensure successful engraftment of donor stem cells.
Living with a Bone Marrow Disorder
- Receiving a diagnosis of a bone marrow disorder can be emotionally challenging, but many individuals successfully manage their condition and maintain a meaningful quality of life.
- Regular medical follow-up remains essential. Routine blood testing allows healthcare providers to monitor disease activity, evaluate treatment effectiveness, and identify complications early.
- Patients can help reduce infection risk by practicing good hand hygiene, staying current with recommended vaccinations, avoiding exposure to contagious illnesses when possible, and promptly reporting signs of infection.
- Nutrition plays an important role in supporting overall health. A balanced diet rich in fruits, vegetables, lean proteins, whole grains, and essential nutrients helps maintain strength and support recovery. Patients should discuss any dietary restrictions or concerns with their healthcare providers.
- Physical activity, when medically appropriate, can improve energy levels, cardiovascular health, muscle strength, and emotional well-being. Exercise programs should be individualized based on disease status and physical capabilities.
- Emotional and psychological support is equally important. Many patients benefit from counseling services, support groups, educational resources, and strong social support networks.
Bone Marrow Disorders in Children
- Although many bone marrow disorders occur more frequently in adults, children can also be affected by a variety of inherited and acquired conditions.
- Inherited bone marrow failure syndromes often present during childhood and may be associated with developmental abnormalities, growth concerns, and increased cancer risk.
- Childhood leukemia is the most common pediatric cancer and remains one of the most significant bone marrow disorders affecting children. Advances in treatment have dramatically improved survival rates over recent decades.
- Pediatric patients require specialized diagnostic approaches and treatment plans designed to address both immediate medical needs and long-term developmental considerations. Multidisciplinary care involving pediatric hematologists, oncologists, nurses, nutritionists, and psychosocial specialists is often essential.
Prevention and Risk Reduction
- Not all bone marrow disorders can be prevented, particularly those caused by inherited genetic mutations or spontaneous cellular changes. However, certain strategies may help reduce risk and promote overall bone marrow health.
- Limiting exposure to toxic chemicals such as benzene and following workplace safety guidelines can reduce the risk of environmentally related marrow damage.
- Avoiding unnecessary radiation exposure and adhering to recommended safety precautions during medical or occupational procedures may also be beneficial.
- Maintaining overall health through balanced nutrition, regular exercise, adequate sleep, and routine medical care supports optimal immune and hematologic function.
- Individuals with strong family histories of inherited bone marrow disorders may benefit from genetic counseling to better understand potential risks and screening options.
- Most importantly, recognizing symptoms early and seeking timely medical evaluation can lead to earlier diagnosis and improved treatment outcomes.
Understanding Prognosis and Long-Term Outlook
- The prognosis for bone marrow disorders varies widely depending on the specific condition, disease stage, genetic characteristics, treatment response, age, and overall health.
- Some disorders remain stable for many years with careful monitoring and minimal intervention. Others require intensive treatment but can achieve long-term remission or cure.
- Advances in molecular diagnostics allow physicians to better predict disease behavior and personalize treatment strategies. Improved supportive care, targeted therapies, immunotherapy, and transplantation techniques have significantly enhanced survival rates for many conditions.
- Ongoing monitoring remains essential even after successful treatment because some disorders can recur or evolve over time.
Recent Advances in Bone Marrow Disease Treatment
The field of hematology has experienced remarkable progress in recent years.
- Genomic profiling now enables physicians to identify specific mutations driving disease development, allowing more precise diagnosis and treatment selection.
- Next-generation targeted therapies continue to improve outcomes while reducing treatment-related toxicity compared with traditional approaches.
- Immunotherapy has emerged as a powerful tool for certain blood cancers, helping the immune system recognize and eliminate abnormal cells more effectively.
- Gene therapy research offers exciting potential for inherited bone marrow disorders by addressing disease-causing genetic abnormalities at their source.
- Advancements in stem cell transplantation techniques have improved donor matching, reduced complications, and expanded treatment options for more patients.
- Together, these innovations are moving healthcare closer to truly personalized medicine, where treatment decisions are tailored to each patient’s unique biological profile.
When to Seek Medical Attention
Medical evaluation should be sought promptly for symptoms such as persistent fatigue, unexplained bruising, recurrent infections, prolonged bleeding, significant shortness of breath, or unexplained weight loss.Urgent medical attention is necessary for high fever, severe infections, uncontrolled bleeding, chest pain, or symptoms suggesting serious anemia.
Individuals with abnormal blood test results should follow up promptly with their healthcare provider, as further evaluation may be required to identify underlying causes.Referral to a hematologist is often recommended when bone marrow disorders are suspected or confirmed.
Conclusion
Bone marrow serves as the foundation of healthy blood production, continuously generating the red blood cells, white blood cells, and platelets that sustain life. When this complex system becomes disrupted, bone marrow disorders can affect virtually every aspect of health, leading to anemia, infections, bleeding complications, and, in some cases, life-threatening cancers.
Early recognition of symptoms, timely diagnostic evaluation, and appropriate treatment are critical for improving outcomes. Advances in molecular diagnostics, targeted therapies, immunotherapy, and stem cell transplantation have dramatically expanded treatment possibilities and provided new hope for patients facing these conditions.While a diagnosis of a bone marrow disorder can be overwhelming, modern medicine offers more effective and personalized treatment options than ever before. Through close collaboration with healthcare providers, ongoing monitoring, and access to specialized care, many individuals can successfully manage their condition and achieve improved quality of life.