Multiple myeloma is a type of blood cancer that develops in plasma cells, a specialized form of white blood cell found in the bone marrow.When these cells mutate and multiply uncontrollably, they crowd out healthy blood cells, produce abnormal proteins (M protein), and cause progressive damage to bones, kidneys, and the immune system.For patients seeking Multiple Myeloma Treatment in Chennai, Kannappa Memorial Hospital offers comprehensive, personalized care delivered by an experienced haematology and oncology team.
Our specialists provide world-class treatment options ranging from early-stage monitoring and targeted therapies to autologous stem cell transplant (ASCT), CAR T-cell therapy, and access to the latest clinical trials. This guide explains everything patients and caregivers need to know about multiple myeloma and why patients across Chennai trust Kannappa Memorial Hospital for advanced cancer care.
What Is Multiple Myeloma?
Multiple myeloma is a type of blood cancer that develops in plasma cells — specialized white blood cells produced in the bone marrow. In a healthy body, plasma cells manufacture antibodies that protect you from infections. When these cells undergo genetic mutations and begin multiplying uncontrollably, they accumulate in the bone marrow, crowd out healthy blood cells, and release an abnormal protein known as M protein (monoclonal protein) — which serves no immune function but gradually damages the kidneys, bones, and immune system.
Signs and Symptoms of Multiple Myeloma
Multiple myeloma is often called a “silent cancer” because it may not cause noticeable symptoms during its early stages. Many patients are diagnosed incidentally during routine blood tests performed for unrelated health concerns. As the disease progresses and more of the bone marrow becomes affected, symptoms become more apparent and can significantly impact daily life.
Early Warning Signs of Multiple Myeloma
In the early stages, symptoms are often mild and may be mistaken for aging, stress, or other common conditions. These early signs can include:
- Persistent tiredness and weakness caused by anaemia as myeloma cells reduce the production of healthy red blood cells
- Mild bone pain, particularly in the lower back, hips, or ribs, that does not improve with rest
- Frequent or recurring infections, such as chest infections or urinary tract infections, due to a weakened immune system
Advanced Symptoms of Multiple Myeloma
As multiple myeloma advances, it can affect several organs and body systems, leading to more serious complications, including:
- Severe back pain or sudden loss of height, which may indicate spinal compression fractures
- Kidney dysfunction, causing swelling in the legs or face, reduced urine output, or frothy urine due to abnormal protein deposits
CRAB Criteria — When Treatment Is Needed
Doctors use the CRAB criteria to determine whether multiple myeloma is causing organ damage and requires active treatment. CRAB stands for:
- C – Calcium elevation: High blood calcium levels caused by bone breakdown
- R – Renal impairment: Kidney damage resulting from abnormal myeloma proteins
- A – Anaemia: Reduced red blood cell production leading to fatigue and weakness
- B – Bone lesions: Bone destruction, fractures, or osteoporosis caused by myeloma cells
The presence of one or more CRAB features usually indicates active multiple myeloma that requires prompt medical intervention. Early evaluation and specialized Multiple Myeloma Treatment in Chennai can help control the disease, manage symptoms, protect organ function, and improve long-term quality of life.
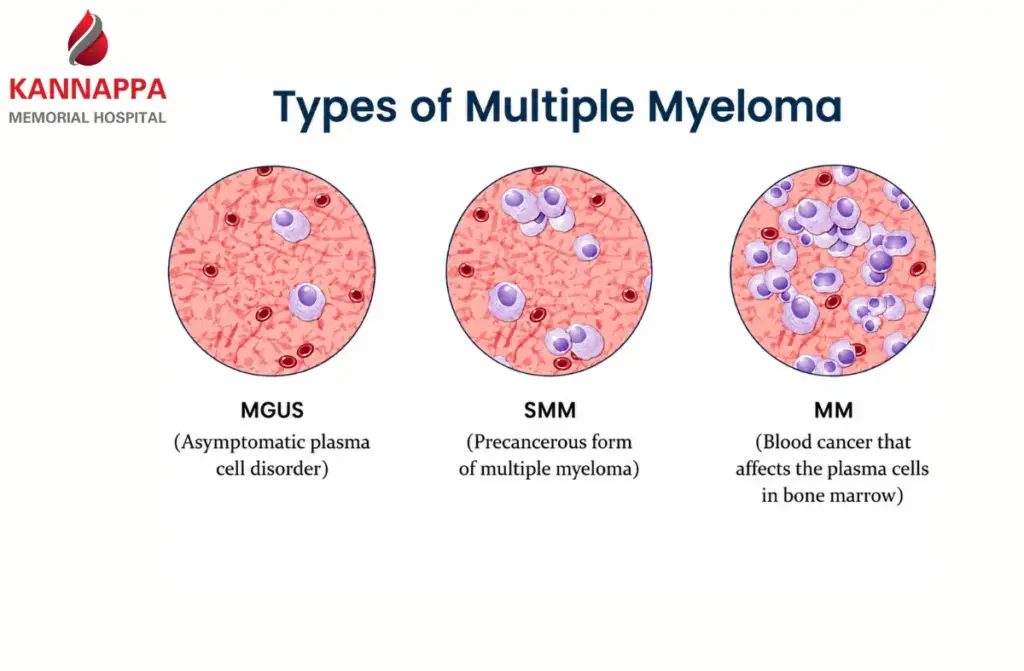
Types and Stages of Multiple Myeloma
Identifying exactly where a patient sits on the disease spectrum determines whether active treatment, close monitoring, or watchful waiting is appropriate.
- Active Multiple Myeloma: Full disease with CRAB features — bone damage, kidney impairment, anaemia, or hypercalcaemia. Requires immediate treatment.
- Solitary Plasmacytoma: A single plasma cell tumour in one bone or soft tissue, without systemic spread. Often managed with radiation; carries a 5-year survival rate of 82.1%.
- MGUS (Monoclonal Gammopathy of Undetermined Significance): A pre-cancerous condition where a small abnormal protein appears in the blood but causes no symptoms or organ damage. Requires regular monitoring as it can progress to active myeloma.
- Smoldering Multiple Myeloma (SMM): An early form of multiple myeloma where abnormal plasma cells and M protein levels are higher than normal, but no symptoms are present. Regular follow-up is essential, and some higher-risk patients may be considered for early treatment or clinical trials.
Causes and Risk Factors
The exact cause of multiple myeloma remains unclear, and researchers continue to study the genetic and environmental factors that contribute to the disease. Multiple myeloma develops when plasma cells in the bone marrow undergo genetic changes that cause them to grow and multiply uncontrollably.
- Age: Age is one of the strongest risk factors for multiple myeloma. Most patients are diagnosed between the ages of 65 and 70, and the disease is uncommon in individuals younger than 40 years.
- Sex: Multiple myeloma occurs more frequently in men than in women. Studies show that men are approximately 1.5 times more likely to develop the disease.
- Race and Ethnicity: People of African descent have a significantly higher risk of developing multiple myeloma compared with other populations. Research indicates that the incidence rate is more than twice as high in this group.
- Family History: Individuals with a close family member, such as a parent, sibling, or child, who has been diagnosed with multiple myeloma may have a higher risk of developing the disease. While most cases occur without a clear hereditary link, family history is considered an important risk factor.
- Obesity: Excess body weight has been linked to a higher risk of multiple myeloma. Obesity may contribute to chronic inflammation and other biological changes that can promote cancer development.
Diagnosing Multiple Myeloma in Chennai
Accurate diagnosis is essential for determining the stage of multiple myeloma and developing an effective treatment plan. At leading cancer centres in Chennai, specialists use a combination of blood tests, urine tests, imaging studies, and bone marrow examinations to confirm the diagnosis and assess the extent of the disease.
Common diagnostic tests include:
- Blood tests to detect M protein, assess kidney function, calcium levels, and blood cell counts
- Urine tests to identify abnormal proteins known as Bence Jones proteins
- Bone marrow biopsy to evaluate the presence and percentage of abnormal plasma cells
- Imaging scans such as X-rays, CT scans, MRI, or PET-CT scans to detect bone damage and lesions
- Genetic and molecular testing to identify specific chromosomal abnormalities that help guide treatment decisions
Early and accurate diagnosis enables specialists to determine disease severity, identify potential complications, and recommend the most appropriate Multiple Myeloma Treatment in Chennai for each patient. Timely evaluation can significantly improve treatment outcomes and quality of life.
Staging and Prognosis
Once multiple myeloma is diagnosed, doctors determine the stage of the disease to assess its severity, guide treatment decisions, and estimate prognosis. The most commonly used system is the Revised International Staging System (R-ISS), which considers blood markers, genetic abnormalities, and disease characteristics.
The R-ISS classifies multiple myeloma into three stages:
- Stage I: Lower-risk disease with favorable prognostic factors and generally better treatment outcomes.
- Stage II: Intermediate-risk disease with characteristics that fall between Stages I and III.
- Stage III: Higher-risk disease associated with more aggressive features and a greater likelihood of complications.
Prognosis varies among patients and depends on several factors, including disease stage, genetic profile, age, overall health, kidney function, and response to treatment. Advances in targeted therapies, immunotherapy, and stem cell transplantation have significantly improved survival rates and quality of life for many patients with multiple myeloma.
Why Choose Kannappa Memorial Hospital for Multiple Myeloma in Chennai?
Kannappa Memorial Hospital offers comprehensive multiple myeloma care through a combination of experienced specialists, advanced diagnostics, and personalized treatment plans. As a dedicated haematology and oncology centre in Chennai, the hospital focuses on delivering evidence-based care while supporting patients throughout every stage of their treatment journey.
Key Reasons to Choose Kannappa Memorial Hospital
- Specialized Multiple Myeloma Team – Experienced haematologists and oncologists provide expert diagnosis, treatment, and long-term disease management.
- Advanced Diagnostic Facilities – Access to modern testing, including bone marrow evaluation, FISH cytogenetics, and MRD (Minimal Residual Disease) testing for accurate diagnosis and monitoring.
- Comprehensive Stem Cell Transplant Services – Full bone marrow transplant programme offering both autologous and allogeneic stem cell transplantation.
- Access to Advanced Therapies – Availability of the latest treatment approaches, including targeted therapies, immunotherapies, clinical trials, and emerging options such as CAR T-cell therapy.
- Multidisciplinary Care Approach – Collaborative treatment planning involving specialists from haematology, oncology, nephrology, radiology, pathology, and supportive care services.
- Personalized Treatment Plans – Every patient receives an individualized care plan based on disease stage, genetic profile, overall health, and treatment goals.
- Dedicated International Patient Support – Assistance for patients travelling from other cities and countries, including treatment coordination and logistical support.
- Holistic Patient Care – Comprehensive supportive services, including pain management, nutritional guidance, psychological counselling, rehabilitation, and survivorship care.
With a commitment to clinical excellence and compassionate care, Kannappa Memorial Hospital strives to provide advanced multiple myeloma treatment and improve the quality of life for patients and their families.
Complications of Multiple Myeloma
Without appropriate management, multiple myeloma causes serious complications:
- Bone destruction and fractures: Myeloma cells trigger aggressive bone breakdown. The spine is particularly vulnerable — spinal cord compression is a medical emergency requiring urgent treatment.
- Kidney failure: Abnormal M protein deposits can harm the kidney tubules and impair their ability to filter waste from the blood. This is one of the most frequent and serious complications seen in the condition.
- Severe infections: Myeloma depletes normal antibody-producing cells, severely impairing immune defences.
- Hyperviscosity syndrome: Excess M protein thickens the blood, causing blurred vision, headaches, and spontaneous bleeding.
- Amyloidosis: Abnormal proteins deposit in organs (heart, kidneys, liver), causing multi-organ damage over time.
Living With Multiple Myeloma
Living with multiple myeloma involves ongoing medical care, healthy lifestyle choices, and emotional support. Many patients can maintain a good quality of life with proper treatment and regular follow-up.
- Nutrition and Exercise: A balanced diet rich in calcium, vitamin D, and protein supports bone health and overall wellness. Regular low-impact exercise can help improve strength, mobility, and energy levels.
- Mental Health and Support: Managing multiple myeloma can be emotionally challenging. Counseling, support groups, and family support can help reduce stress and improve emotional well-being.
- Long-Term Monitoring After Remission: Consistent follow-up appointments are important to track recovery progress and identify any early signs of the disease returning.These may include blood tests, SPEP monitoring, imaging scans, and MRD testing when required.
Prevention and Risk Reduction
Currently, there is no established or proven method to prevent multiple myeloma.However, practical steps to reduce modifiable risk include:
- Maintaining a healthy body weight
- Avoiding unnecessary radiation exposure
- Not smoking
- If diagnosed with MGUS — adhering to your monitoring schedule without gaps, as early detection of progression maximises treatment options
When to Seek Medical Attention
Seek evaluation at Kannappa Memorial Hospital if you experience any of the following:
- Unexplained Weight Loss: Losing weight without changes in diet or exercise may be a warning sign of an underlying medical condition.
- Persistent or Unexplained Bone Pain: Ongoing pain in the back, ribs, hips, or other bones may indicate bone involvement and should not be ignored.
- Recurrent Infections: Frequent infections or illnesses that are slow to resolve despite treatment may signal a weakened immune system.
- Extreme Fatigue or Weakness: Persistent tiredness that interferes with daily activities can be a sign of anemia or other underlying health concerns.
- Fractures After Minor Injury: Bones that break easily from minor falls or without a clear cause may indicate weakened bone strength.
- Numbness, Tingling, or Limb Weakness: These symptoms can occur when nerves are affected and require prompt medical evaluation.
Patient Testimonials
Dr. Gopinath at Kannappa Memorial Hospital is an exceptional hematologist. From my very first appointment, I felt like I was in incredibly capable and caring hands. He took the time to really listen to my concerns and explain my diagnosis in a way that was both informative and reassuring. What impressed me most was his genuine empathy and compassion.I’m so grateful for his expertise and the excellent care I received. I highly recommend Dr. Gopinath to anyone seeking a compassionate and skilled hematologist
Conclusion
Multiple myeloma is a complex but increasingly treatable blood cancer. Advances in quadruplet induction regimens, autologous stem cell transplantation, CAR T-cell therapy, and bispecific antibodies have transformed what was once a uniformly poor prognosis into a condition in which long-term remission and for some patients, many years of excellent quality of life is achievable.
At Kannappa Memorial Hospital, our integrated approach to multiple myeloma care combines world-class diagnostic precision, evidence-based treatment, and compassionate patient support because every patient deserves the best possible chance at a meaningful life beyond diagnosis.
Read more: Lymphoma Cancer Symptoms